Vomiting can be a sign of an underlying condition. Treatment of vomiting must be done for the underlying cause.
To prevent electrolyte imbalance and dehydration, however, it is important to start symptomatic treatment immediately.
Vomiting refers to the voluntary expulsion of gastrointestinal contents.
Vomiting can be a sign of many conditions, so antiemetic drugs are not the best option.
It is important to determine the root cause of the vomiting before you can treat it.
These drugs may not work permanently. Therefore, it is recommended that you treat the underlying condition simultaneously.
What class of medicine is used to treat nausea?
-
Anticholinergic agents
-
Antihistamines
-
Dopamine receptor antagonists
-
Butyrophenones
-
Benzamides
-
An antagonist of the serotonin receptor
-
An antagonist of neurokinin receptors
-
Glucocorticoids
-
Cannabinoids
-
Benzodiazepines
Anticholinergic agents for the treatment of vomiting:
Scopolamine, an anticholinergic agent that is used for vomiting treatment, is the most well-known. Scopolamine is used to prevent motion sickness.
Antihistamines for Vomiting:
Motion sickness is the main reason antihistamines are used. Sedation is the most significant side effect of antihistamines.
Antihistamines are commonly used as antiemetics.
-
50 mg of Dimenhydrinate (Gravinate), every four hours
-
Diphenhydramine (Avil), 25 - 50mg four times daily
-
Cyclizine (50mg IM every four hour)
-
Meclizine (25-50 mg taken orally once daily).
-
Promethazine (25 mg to 25 mg orally, or IM every four hour)
Dopamine receptor antagonists as antiemetic:
Dopamine receptor antagonists include:
- Phenothiazines
- Butyrophenones
- Benzamides
Phenothiazines
The most common antiemetic in this class is Prochlorperazine, also known as Compazine.
It can be taken intramuscularly orally at a dose of 5-10 mg every six to eight hours.
It can be used to treat vomiting in various gastrointestinal conditions and mild to moderately-emetogenic chemotherapy.
Chlorpromazine (Thorazine), 10-25 mg orally every 4 to 6 hrs, or intravenous every 3 to 4 hours.
Phenothiazines can cause extrapyramidal side effects such as dystonia or tardive dyskinesia.
The treatment of acute dystonia can be done with diphenhydramine and benzodiazepines (25 to 50 mg intramuscularly, or slowly intravenously).
Hypotension, especially for elderly patients, can also be an adverse effect of intravenous injections.
Butyrophenones:
Droperidol (inapsine), and haloperidol can be used to calm patients and pre-procedural sedating agents.
However, they also have antiemetic and prevent nausea and vomiting from occurring after surgery.
Butyrophenones have extrapyramidal side effects. However, there is a dose-dependent risk for QT prolongation or torsades De points in patients older than 65 and those who take other medications that affect QT interval. Because of safer alternatives, these agents are less frequently used.
Benzamides
This group includes the major drug,metoclopramide.
Benzamides block the D2 receptor in the central part of the brain, as well as weak 5HT3 blocking properties.
It increases the release of Acetylcholine from the Neuromuscular Junction by stimulating the cholinergic receptors in the gastric smooth muscle.
The US FDA has issued a Black Box Warning about the risk of irreversible tardive disorders with long-term high doses and prolonged use.
Metoclopramide:
It has a mild antiemetic action, increases gastric motility, and raises the tone of lower esophageal.
Metoclopramide can be used to treat delayed emesis caused by cisplatin.
It can also be used in combination with other anti-emetic drugs. It was previously used with diphenhydramine and steroids before chemotherapy.
Neurologic side effects are the most common side effects of metoclopramide.
These include tardive dyskinesia, dystonia and akathisia.
Domperidone (Motilium):
Another D2-receptor blocking drug with selective peripheral activity in upper gastrointestinal tract.
Domperidone is not able to cross the blood-brain border, so it is superior than metoclopramide (because it does not have the neurologic side effects).
Serotonin Receptor Antagonists for the treatment of vomiting:
The main purpose of the 5 HT3 receptor antagonists is to treat chemotherapy-induced nausea.
The four approved serotonin receptor antagonists are dolasetron (granisetron), ondansetron (and palonosetron).
Palonosetron has an extended half-life and is more effective than other drugs, especially when taken in combination with dexamethasone.
Both intravenous and oral formulations have similar efficacy and should be administered prior to chemotherapy.
The most common adverse effect is headache, followed by constipation, dizziness, asthenia, and constipation.
Dolasetron, granisetron and ondansetron can have an effect on the heart as shown by changes in ECG intervals.
These agents can cause QT prolongation or fatal cardiac arrhythmias in patients who receive them.
The US Food and Drug Administration (FDA), recommends that patients receiving these medications should monitor their EKG, especially if they have concomitant potassium and magnesia deficiency or are taking other drugs that prolong QT intervals or have CHF.
Neurokinin receptor antagonists as antiemetics:
Aprepitant and Fosaprepitant:
The new antiemetic drugs were originally introduced to prevent chemotherapy-induced vomiting.
They prevent acute and delayed vomiting, unlike the serotonin antagonists.
They work best when combined with dexamethasone and serotonin receptor antagonists.
Glucocorticoids are strong antiemetic drugs:
Glucocorticoids are known for their strong antiemetic abilities.
These drugs can be used together with metoclopramide and serotonin receptor antagonists or neurokinin receptor antagonists to treat chemotherapy-induced vomiting.
These settings are often where Dexamethasone can be used as an antiemetic.
Cannabinoids for vomiting:
After some patients discovered that cannabis-like drugs reduced chemotherapy-induced vomiting, they were used as antiemetic medications.
Nabilone, dronabinol and dronabinol can be used as antiemetics. These drugs are superior to prochlorperazine, but have a lower efficacy than metoclopramide.
The two most beneficial side effects for cancer patients are sedation and euphoria, but it is not routinely used due to dry mouth, vertigo and hypotension.
Benzodiazepines as antiemetic drugs:
Alprazolam, lorazepam and metoclopramide have antiemetic qualities and can be helpful for patients with adverse effects from steroids (insomnia), and metoclopramide movement disorders (metoclopramide).
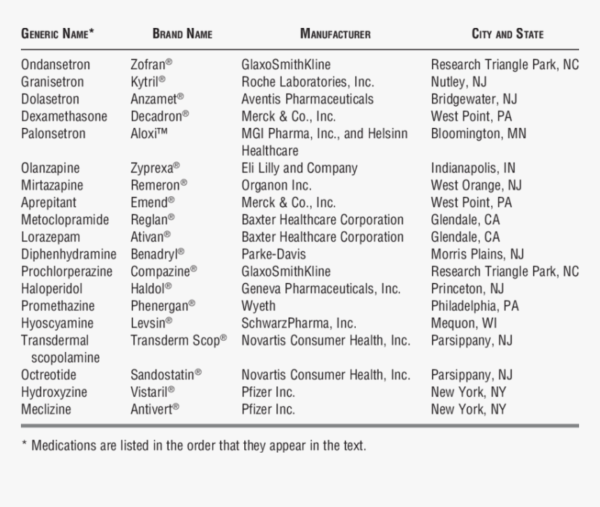
[caption id="attachment_10692" align="aligncenter" width="860"] Summary of drugs used to treat vomiting[/caption]
Summary of drugs used to treat vomiting[/caption]



